Hypertension treatment for chronic kidney disease (CKD)
Hypertensive patients with chronic kidney disease (CKD)
are often prescribed renin-angiotensin (RA) system inhibitors,
such as angiotensin receptor blockers (ARBs) and
angiotensin-converting enzyme (ACE) inhibitors.
This is because the drug has been believed to have a renoprotective effect
by dilating the efferent arterioles of the renal glomeruli and reducing intraglomerular pressure.
Blood pressure is regulated by many factors,
but the most influential is the renin-angiotensin (RA) system of hormones.
Among them, angiotensin II has a strong effect of increasing blood pressure.
ARBs lower blood pressure by blocking angiotensin receptors.
Angiotensin II also
narrows the blood vessels at the exit of the renal glomeruli (efferent arterioles) and
increases the pressure inside the glomeruli (intraglomerular pressure).
As a result, proteinuria increases and contributes to glomerular hyperfiltration.
ARBs also inhibit their action, thus acting protectively on the kidney.
However,
since the glomerular filtration rate decreases,
the serum creatinine level (Cr) may apparently increase.
If there is no increase of 30% or more (if Cr 1.0, Cr 1.3 or more),
it is considered that renal protection can be obtained by continuing to take it.
If >30%, reduce or discontinue for bilateral renal artery stenosis.
Angiotensin-converting enzyme (ACE) is
an enzyme that converts angiotensin I to angiotensin II.
By inhibiting this enzyme activity,
ACE inhibitors suppress the production of angiotensin II and lower blood pressure.
ACE inhibitors, like ARBs, also have renoprotective effects,
so there is a risk of transient creatinine elevation.
ACE inhibitors have also been shown to have cardioprotective effects
inhibition of cardiac remodeling,
prevention of recurrence of myocardial infarction,
improvement in prognosis of heart failure patients, etc..
The difference from ARB is side effects
such as “dry cough” and “discomfort in the pharynx”.
However,
ischemic nephropathy due to renal artery stenosis and renal arteriosclerosis is common,
especially in the elderly.
It has been pointed out that there is a risk of hyperkalemia and elevation of Cr.
Calcium channel blockers with low risk of decreased renal blood flow
appear to be desirable as first-line antihypertensive drugs
for chronic kidney disease (CKD) patients aged 75 years and older.
Recently,
sacubitril valsartan sodium hydrate, an angiotensin receptor neprilysin inhibitor (ARNI),
has emerged as a heart failure drug.
ARNI is a combination drug of a neprilysin inhibitor and an ARB.
It is a single crystal complex
in which sacubitril, a neprilysin inhibitor prodrug, and valsartan, an ARB,
are combined in a 1:1 molar ratio in one molecule,
and rapidly dissociate into sacubitril and valsartan after oral administration.
It is expected to be effective as a new antihypertensive drug.
In addition,
if hyperkalemia is observed,
it is necessary to adjust the amount of potassium contained in food
so as not to cause arrhythmia or cardiac arrest.
In particular,
attention should be paid to non-dietary potassium intake.
Fruits contain a lot of potassium, and
one banana contains 454mg of potassium,
one apple contains 394mg, and
even a small mandarin orange contains 120mg.
It’s dangerous to eat a lot of fruit
although it’s good for your health,
it’s something you’ve been eating for a long time,
it’s seasonal, and
it’s just something you’ve had the chance to eat.

Check the potassium content of commercially available beverages
especially vegetable juices and vegetable juices
before drinking.
Tomato juice (546 mg potassium per 200 ml),
100% orange juice (378 mg potassium per 200 ml), and
milk (300 mg potassium per 200 ml) should be avoided.
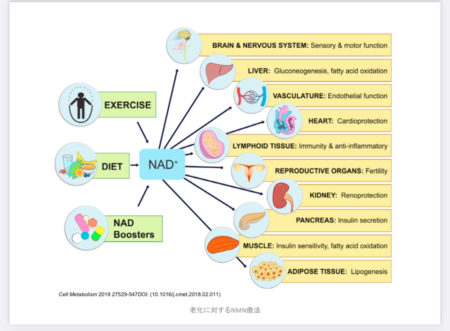
In addition, at our clinic,
we expect the effects of NMN (nicotinamide mononucleotide)
to lower blood pressure (cardioprotection, blood flow improvement)
and renal function improvement (renal protection, blood flow improvement).